More AI Doesn't Always Mean Better Healthcare
Artificial intelligence is expanding at an astonishing pace, consuming more money, energy, and computing power than ever before. Yet while we debate whether AI will replace physicians or eliminate jobs, another challenge is quietly growing in the background: the rapidly escalating financial and environmental cost of AI.
AI token consumption is skyrocketing, but measurable business value is often struggling to keep pace. Recent reports illustrate the challenge. Uber executives acknowledged that AI spending has accelerated so rapidly that it has become difficult to precisely quantify its return, with Claude Code token costs reportedly reaching approximately $2,000 per engineer (Fortune, 2026).
Axios similarly reports that many enterprises are dramatically increasing AI spending while still struggling to demonstrate a clear return on investment. A company accidentally spent $500 million on Claude licenses in a month after failing to cap usage (Axios, 2026).
Another widely discussed example described an AI developer consuming 1.3 million OpenAI API tokens in a single month, illustrating how quickly costs can spiral when usage is left unchecked (Tom’s Hardware, 2025).
Apparently, AI doesn’t just hallucinate—it invoices too.
Why More AI Doesn't Always Mean Better Care
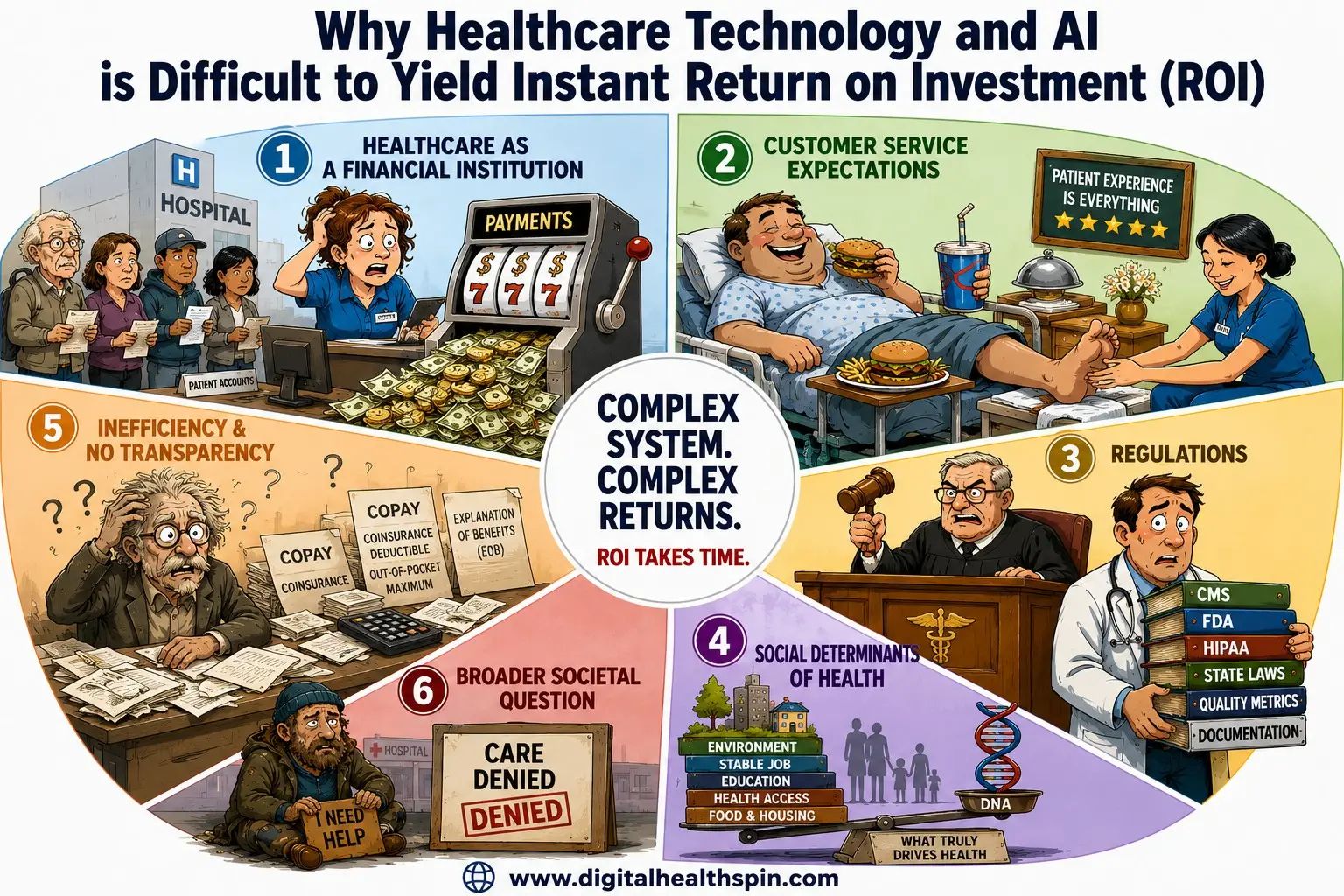
Healthcare is arguably the most complex industry in the economy because it combines elements of nearly every other sector. It manages financial transactions on the scale of major banking institutions, with U.S. national health expenditures exceeding $5 trillion annually (CMS, 2024).
Hospitals and health systems process millions of claims, payments, and reimbursements every day while simultaneously delivering highly regulated clinical care.
Healthcare also has customer service expectations comparable to the hospitality industry. Patients increasingly expect personalized, seamless experiences—almost like checking into a Disney resort—while clinicians are simultaneously expected to deliver life-saving care under significant operational constraints.
Add to that a regulatory landscape resembling aviation or nuclear power, except the rules frequently differ across states, payers, and healthcare organizations.
Perhaps the greatest challenge, however, is that health outcomes depend on much more than biology. They are shaped by an interaction between genetics and the social determinants of health—including education, income, housing, environment, health behaviors, and access to care (WHO, 2023; Office of Disease Prevention and Health Promotion, n.d.).
Our Healthcare sector is also remarkably inefficient. Despite decades of investment in electronic health records, interoperability remains inconsistent, limiting the seamless exchange of patient information across healthcare organizations (ONC, 2024).
In many communities, two hospitals located across the street from one another still struggle to exchange complete patient records—even when using the same electronic health record vendor.
There is also a remarkable lack of transparency throughout the healthcare financing system. Good luck explaining the difference between your deductible, copay, coinsurance, out-of-pocket maximum, prior authorization, and explanation of benefits. By the time most patients figure out which bill they’re supposed to pay, a new one has already arrived.
Finally, healthcare remains deeply divided on one of its most fundamental questions: Is healthcare a basic human right? Until society reaches greater consensus on who should receive care and how it should be financed, every technological innovation—including AI—will face structural barriers to delivering its full potential.
Collectively, these realities make healthcare one of the most difficult industries in which to implement new technology. Simply adding more AI without addressing these underlying structural problems risks making an already complex system even more expensive rather than more effective.
The Real AI Risks in Healthcare
The AI Risk We Face is Sinister and Hidden in Plain Site
Contrary to Hollywood portrayals of rogue machines, today’s AI risks are far less dramatic—but potentially far more expensive.
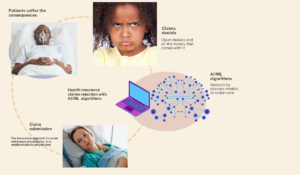
The greatest risks are not machines replacing clinicians; they are widening health disparities, increasing healthcare costs, and expanding the environmental footprint of increasingly energy- and water-intensive data centers.
More importantly, many of healthcare’s biggest challenges are not technological. Inefficient workflows, fragmented health records, poor interoperability, opaque payment models, and unequal access to care are fundamentally human and policy problems. Layering AI onto broken systems without first addressing these foundational issues simply allows expensive inefficiencies to run faster.
Digital therapeutics perfectly illustrate both the promise and the limitations of AI-enabled healthcare. The U.S. Food and Drug Administration has now cleared prescription digital therapeutics for conditions such as generalized anxiety disorder, representing an important milestone for evidence-based digital medicine.
These products demonstrate that software, when rigorously evaluated, can become a legitimate therapeutic intervention.
Unfortunately, many of these innovations are available primarily through employers or commercial health insurance plans. Since approximately 27 million Americans remain uninsured, many of the people who could benefit the most from these technologies may never gain access (CDC, 2025).
It’s a little like inventing the world’s safest self-driving car and then announcing that only people who already own a luxury vehicle are allowed to drive it.
The same concern applies globally. Deploying increasingly sophisticated AI on top of healthcare systems that still cannot exchange information effectively is like installing a Formula 1 engine into a shopping cart. It certainly becomes faster—but not necessarily safer, more efficient, or capable of reaching its destination.
The environmental implications deserve equal attention. Modern generative AI models require enormous computational resources, consuming substantial electricity and water to train and operate. As healthcare organizations rapidly adopt AI, leaders must ask an important question: Are we creating sufficient clinical value to justify the environmental and financial resources being consumed?
Healthcare has always operated under finite resources. Every dollar invested in AI should be done bearing in mind the need for preventive care, workforce development, primary care access, interoperability, or addressing the social determinants of health.
Responsible AI adoption therefore requires more than technical excellence—it requires thoughtful prioritization.
Technology alone rarely fixes broken systems. History has repeatedly shown that digitizing inefficient processes simply creates faster inefficiency. AI is no exception.
"Layering AI onto broken systems without first addressing foundational issues like interoperability simply allows expensive inefficiencies to run faster"
Ahmed-Digital Doc Tweet
"The greatest irony of healthcare AI is that the patients who stand to benefit the most are often the least able to access it. Building revolutionary AI that only the privileged can afford is like inventing the world's safest self-driving car—and then handing the keys only to those who already own a luxury garage."
Ahmed-Digital Doc Tweet
Digital health 360 degrees lens
Healthcare does not have an AI problem—it has a value problem.
AI should not be judged by the sophistication of its algorithms but by its ability to improve patient outcomes, reduce health inequities, lower the total cost of care, make clinicians’ lives easier, and minimize its environmental footprint.
Unless healthcare organizations first improve governance, workflows, interoperability, and transparency, AI risks becoming another expensive layer added to an already fragmented ecosystem rather than the transformative solution many hope it will be.
The winners of the AI era will not necessarily be the organizations deploying the most AI. They will be the organizations whose leaders can distinguish genuine clinical value from expensive hype.
Healthcare executives should resist investing in AI simply because competitors are doing so. Like teenagers learning to ignore peer pressure, organizations need the discipline to avoid buying technology driven by fear of missing out rather than measurable outcomes.
Healthcare organizations do not need more AI; they need better decisions about where AI belongs.
The better question is not:
“How much AI are we deploying?”
“Which AI demonstrably improves patient outcomes, advances health equity, reduces costs, promotes environmental sustainability, and creates measurable value?”
Digital health should not be judged by how intelligent the technology is, but by how intelligently it improves healthcare.
How is your organization deciding where AI belongs—and where it doesn’t?
If your organization is evaluating an AI or digital health solution, reach out to Digital Health 360° Academy at info@digitalhealthspin.com. We help healthcare organizations determine whether emerging technologies are clinically appropriate, operationally feasible, financially sustainable, environmentally responsible, and ultimately worth the investment before implementation.
In Good Health,
The Digital Health 360° Framework™
Your guide to health innovation through:
- Clinical Value
• Health Equity
• Economic Sustainability
• Environmental Sustainability
References:
Anxiety Disorders Association of America. (n.d.). Facts and statistics. https://adaa.org/understanding-anxiety/facts-statistics
Balaskas, A., et al. (2021). The functionality of mobile apps for anxiety. JMIR mHealth and uHealth. https://mhealth.jmir.org
Big Health. (n.d.). Daylight digital therapeutic. https://www.bighealth.com
Calm. (n.d.). Calm app. https://www.calm.com
Chalmers, J. A., et al. (2014). The relationship between heart rate variability and emotion regulation. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC4092363/
Garcia, et al. (2024). Anxiety and cardiovascular risk. PubMed. https://pubmed.ncbi.nlm.nih.gov/38389520/
Headspace. (n.d.). Headspace app. https://www.headspace.com
HRSA. (n.d.). Health workforce shortage areas. https://data.hrsa.gov
Meru Health. (n.d.). Meru Health program. https://www.meruhealth.com
Amwell. (n.d.). SilverCloud digital mental health platform. https://silvercloud.amwell.com
AbleTo. (n.d.). Sanvello app. https://www.sanvello.com
Wysa Ltd. (n.d.). Wysa app. https://www.wysa.com
Woebot Health. (n.d.). Woebot app. https://woebothealth.com